NAM - Acid-Base-buffer measuring by Jörgensen
In literature there are many theories on acid-base diagnostics. Measuring the pH of urine is not very helpful. If the kidney does not let acid out of the body, you will find a basic urine but in front of you you have an acidified patient. The pH measurement of the blood does not help either, because the pH value of the blood is always normal, unless the patient is on the way to the intensive care unit with flashing blue light.
But something happened between „healthy“ and „flashing blue lights“:
The body lost the ability to control the pH-value and keep it in the norm. But this causes the buffer capacity of the blood. Therefore, the question does not have to focus on the urine- or blood pH value, but on the buffer capacity.
With a little effort the buffer capacity can be determined with the NAM acid-base set. In the literature, the method has been classified as „determination of the buffer capacity according to Jörgensen“.
This is a blood test that cannot be performed by the patient himself.

pH-value
The pH-value, measured with a semi-micro-electrode, immediately after taking blood should normally be between 7.35 an 7.55. Deviations are life-threatening and are therefore prevented by the organism due to the buffering capacity of the blood. That is why the pH-value is only important in extreme emergency situations. The buffer capacity of the blood is more important.
Buffer capacity
The buffer capacity is between 47-56 mmol/L and can be determined with a simple,fast and inexpensive titration. A decrease in the buffer capacity at a normal pH value is known as „latent acidosis“ which is an early warning signal for many modern metabolic diseases. It announces a drop in pH long before the emergency situation occurs. The buffer capacity which is determined with our method can be converted into the base excess (BE) of the blood-gas-automat and has not only the same, but a more extensive value. In contrast to the blood-gas-automat, it also contains the nonvolatile acids and bases, for example lactic acid, which is the actual power limiter in geriatrics and sports medicine.
Tissue acidity
The usual distinction between blood- and tissue acidity is not entirely correct, it is better to differentiate between extra- and intracellular acidity. The intracellularly hidden acidic valences elude renal elimination as well as the usual pH measurement, which always measures only extracellularly. Therefore it is the most dangerous type of acidification and should be recognized in time.
- 5-10 ml of blood is required, preferably on an empty stomach, without previous physical exertion and without stasis
- Put the blood in heparin coated capillary tubes
- For the measurement use 1 ml of the blood in a test tube, the rest is centrifuged to collect plasma.
- Measure the pH value oft he whole blood with a pH meter and a glass electrode single-rod measuring cell
- Then 0.1ml of the titration solution is added 5-6 times with a microliter pipette
- The same series of measurements is repeated with 1 ml of plasma
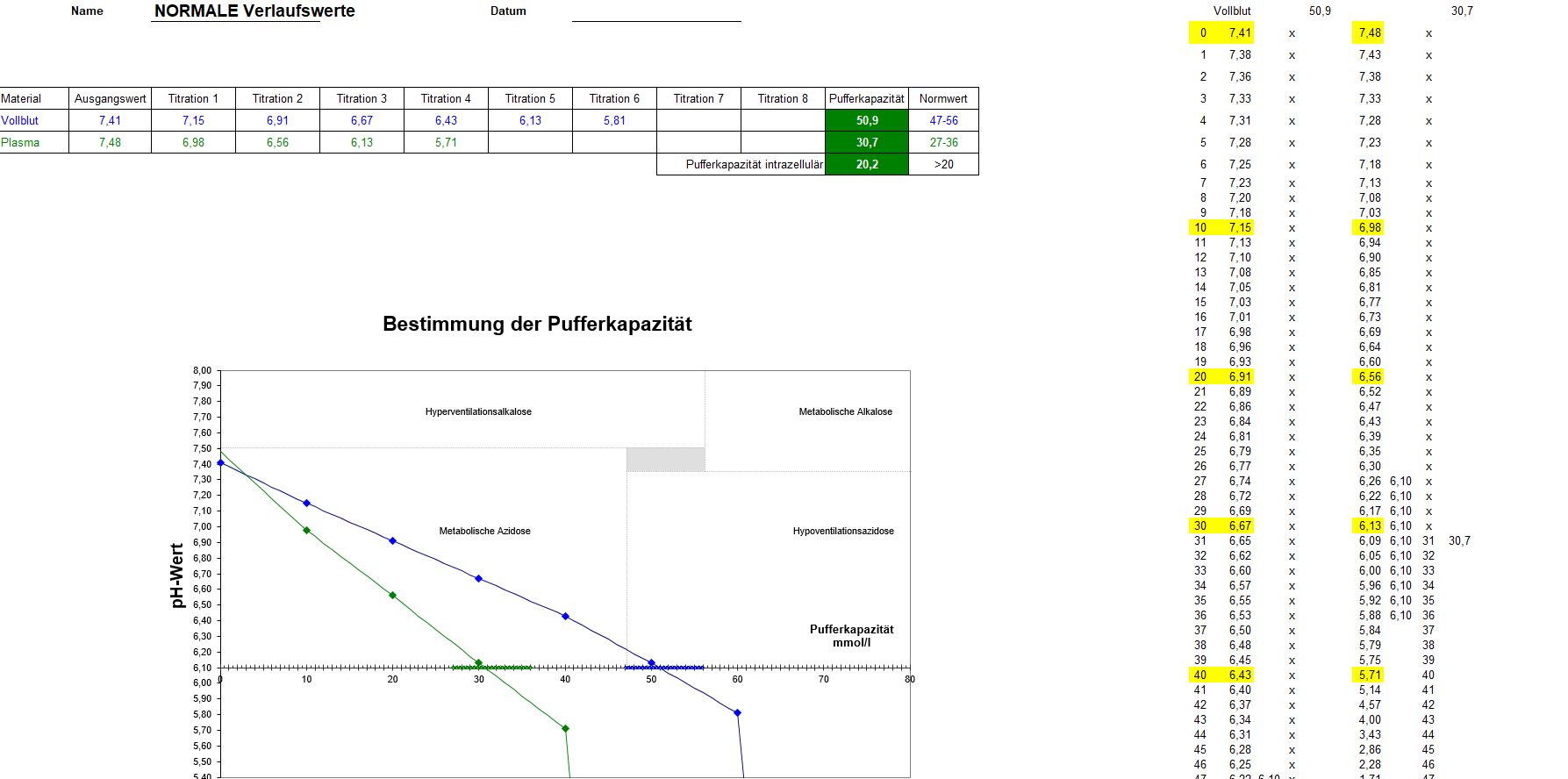
- After each addition the pH values are entered in a nomogram (Excel table, see fig.)
- At the intersection of the resulting measurement curve with the abcsissa at pH 6.1, the buffer capacity can be read in mmol/ L(corresponding to 8.4% sodium hydrogen carbonate solution in ml)
- The time required for such an examination is approximately 10-15 minutes
To enlarge you can click on the picture
A therapy concept can be calculated from the result of the main bicarbonate buffer
Exampe:
A determined base deficit of -5 (base excess) with a body weight of 80kg results in:
-5 x 0,3 x 80 = 120ml 8,4% sodium bicarbonate solution buffer deficit
The pH buffer capacity (mmol/L) ,of which the results deviate from the norm, will be „filled up“ with 8,4% sodium bicarbonate solution. Mostly there are deficits between 100 to 300 ml after the taken measurements (blood titration).
A confirmatory measurement after 4-6 weeks recommendable.
Commonly the human system works excellently with complete health. The acids are completely released and the acid-base balance is fully functional.
An incorrect and too high-protein diet, fast food and a lack of fluid intake, environmental and pleasure poisons, distress situations up to „modern burnout“, a lack of physical exercise with reduced breathing and lactate formation lead to a predominance of the acidifying factors.
A reduction in the buffer capacity can be referred to as „latent acidosis“. Latent, because it slumbers and, according to the conventional view, is not manifest yet. In fact, however, local tissue acidosis with its consequences such as ischemia, infarction, apoplexy, osteoporosis, degeneration of the collagenous connective tissue, pancreatic insufficiency, etc. is favoured.
The consumption of the basic buffer substances in the blood rises but there is still no change in the pH value. In addition, there is increasing demineralization and with it an increased risk of osteoporosis.
At least an aggravation of the already existing hyperacidosis should be restricted.
